Value-based care is won between the visits
The visit is a snapshot. Outcomes are decided in the weeks between, where blood pressure drifts and medications lapse. That's the care a practice built around appointments can't run. ITERA runs it for you.
Refer your chronic patients to ITERA HEALTH. We manage them between visits, under your direction. You keep your practice as it is, and Medicare pays you to stay in the loop.
The visit is a snapshot. Outcomes are decided in the weeks between, where blood pressure drifts and medications lapse. That's the care a practice built around appointments can't run. ITERA runs it for you.
ITERA participates in the Medicare ACCESS model, where payment follows measurable health improvement, not volume. You don't have to participate to benefit. You refer, ITERA takes on the outcome-aligned care, and you bill the new co-management payment for coordinating along the way.
ITERA carries the outcomes risk. You keep your practice, your patients, and your billing.
Most practices run chronic care as a patchwork: CCM on one vendor, RPM on another, each with its own login and experience. BrickL runs all of it on one infrastructure.
Lighter-touch patients need prevention and steady management. More acute patients, with hospitalization and readmission risk, high ER utilization, and multiple uncontrolled conditions, need far more intensity of care and monitoring. The same platform runs both, scaling up to structured programs like CCM, RPM, BHI, and TCM, without switching systems.
The care model changes underneath the patient. What they see stays the same.
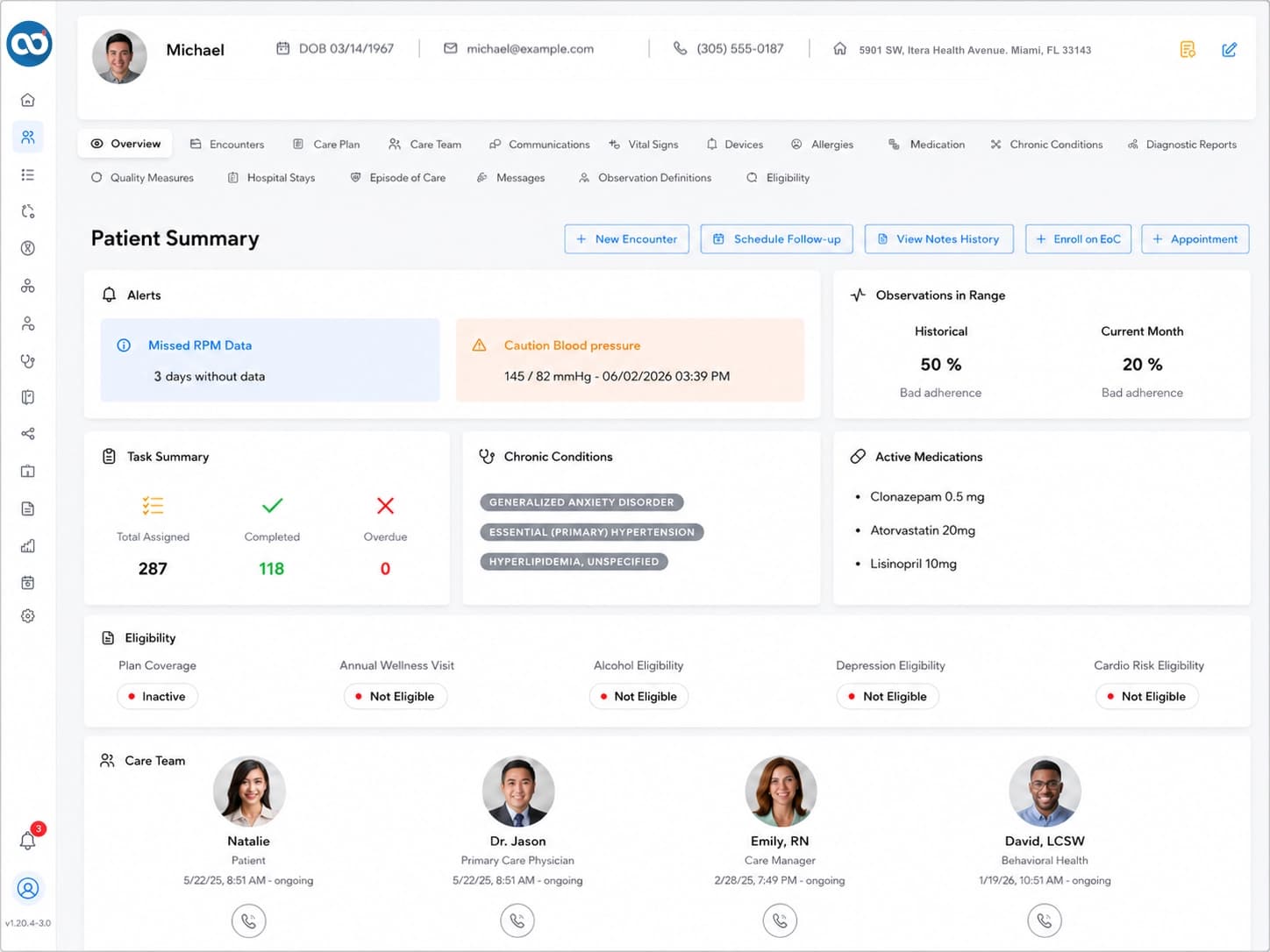
Your care plan drives it. BrickL assembles the care network, coordinates across every provider, and pulls physiologic and patient-reported measurements continuously. Analytics flag where to intervene; quality gaps close before they become misses. ADT feeds catch hospital events and automate transitional care. No new system for your staff to run.
BrickL connects clinician, patient, caregiver, and care manager in one ecosystem of apps. A care plan can be adjusted the moment something changes, not at the next visit. The family stays activated in the same place; your care team acts on what they report instantly.
BrickL ingests the patient's complete Medicare claims history through CMS Blue Button, every encounter and prescription across every provider. A patient-up view no single EHR can produce, and it makes the updates you get back richer than your own chart.
 Consent on file
Consent on fileA patient-up view no single EHR can produce — richer than your own chart.
Measured across our own high-risk cardiovascular Medicare patients over two years. CMS illustrates the ACCESS target as a 10 mmHg reduction. We're already there.
A reduction this size is associated in the literature with lower heart failure, stroke, and major cardiovascular event risk.
Projected implications of the measured result, not separately measured. (Ettehad 2016; Whelton 2024.)
We'll show you how referral and co-management work, and how ITERA runs longitudinal care for your chronic patients.







